Complaint
The risk of iliotibial band syndrome can be reduced by paying attention to the following:
The most common cause is overload (training too much, too often and too hard). This is a pitfall, especially at the start of the season or when returning from an injury. A good training structure is important, whereby the scope of the training is first expanded (the number of hours) and only then the intensity (intensive forms of exercise with a lot of running work).
Due to its damping effect, forest soil is an ideal surface to walk on, especially when you are just starting to walk.
Participating in extreme sporting challenges gives a kick! However, don’t sell yourself short and make sure you start your sports preparation early enough. Being well trained at the start is essential to prevent injuries.
Choose sports shoes that are suitable for the personal running style and foot shape. Good advice from the specialist shop is very valuable here. The average life of a sports shoe is 500 to 750 kilometers. After this, it quickly loses its shock-absorbing effect.
Sometimes the body has certain shortcomings (think X and O legs) that can cause an injury. When these factors are recognized and corrected in time, unnecessary injuries are prevented.
Condition
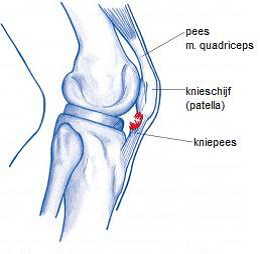
The knee tendon (patellar tendon) comes from the thigh muscle (m. quadriceps) and attaches to the tibia. The kneecap (patella) is embedded in the patellar tendon. Repetitive movements that require extreme force from the thigh muscles can cause irritation in the patellar tendon. This is accompanied by swelling, inflammation and tissue breakdown. An irritation of the patellar tendon is usually localized just below the kneecap, but it also occurs at the attachment to the tibia.
This injury is also popularly referred to as the jumper’s knee. This name does not come out of the blue, because the injury mainly occurs in sports that involve a lot of jumping, such as volleyball and basketball.
Causes
A number of underlying factors can cause a jumper’s knee in hand
to work. The complaints can be the result of properties related to the body (= intrinsic), but environmental factors (= extrinsic) can also play a role.
Intrinsic:
- Knocked legs or a leg length difference cause an asymmetrical load on the patellar tendon
- Flat foot. This causes the lower leg to sink inwards and an X-position of the knee is caused
- Weak medial vastus. Due to weakness of the muscle on the inner side of the thigh (vastus medialis), the knee tends to inward and the patellar tendon is loaded in an unnatural direction
- Shortened thigh muscles. Due to the shortening of the thigh muscles, especially the muscles on the outside of the thigh, the kneecap experiences an outward force
- Overweight. There is an increased load on the knee joint
Extrinsic:
- Overload: frequent running and jumping. Volleyball and basketball in particular are stressful sports for the patellar tendon
- Footwear: old soles with little cushioning or shoes that are unsuitable for the training surface
- Walking on a hard surface
Treatment
Correcting intrinsic and extrinsic factors is a first step. For example, measuring insoles, using braces or adjusting footwear and surface.
- Eccentric exercises of the thigh muscles, in which the muscle is lengthened during active contraction.
- Exercise therapy aimed at strengthening the thigh muscles, in particular the vastus medialis.
- Stretching exercises of the thigh muscles.
- Exercises should be performed once or twice a day for 12 weeks (or shorter if the complaint has disappeared earlier). Research has shown that after 3-6 months 50-60% of athletes have returned to their old level
- Keeping ice on the most painful spot for at least 10 minutes after the exercises reduces blood flow and also reduces the inflammatory response
Medicijnen:
In de acute fase kunnen ontstekingsremmers (diclofenac of ibuprofen) de klachten verminderen. Het doel is om de knie tot rust te brengen waarna kan worden gestart met oefentherapie.
In het verleden werden regelmatig injecties gegeven met corticosteroïden (ontstekingsremmers). In een enkel geval kan dit zinvol zijn. Het nadeel is echter dat de injecties vaak maar tijdelijk effect hebben, en dat het peesweefsel door de ontstekingsremmer verzwakt raakt en mogelijk zelfs zou kunnen scheuren.
Andere medicamenteuze behandelingen zijn aprotinine injecties, polidocanol injecties en nitraatpleisters. Met deze therapievormen zijn goede resultaten gemeld, maar het wetenschappelijke bewijs is nog erg mager.
PRP injecties:
Dit is een veelbelovende techniek waarbij bloed van de patiënt wordt afgenomen wat vervolgens bewerkt wordt. De zo verkregen lichaamseigen groeifactoren kunnen in de pees worden ingespoten waar zij voor herstel van de pees zorgen.
Operatie:
Bij een operatie wordt het beschadigde peesweefsel weggehaald. Daarnaast kan de pees voor een deel ingesneden worden, hierdoor verlengt de pees. Nadeel van de operatie is een lange herstelperiode en succes is niet altijd gegarandeerd.
Jumpers knee en sport
Neem (relatieve) rust: breng de sportbelasting terug tot een niveau waarop de klachten niet worden uitgelokt. Kies voor alternatieve sportactiviteiten om de conditie op peil te houden, zoals fietsen of de crosstrainer.
Bij duidelijke vermindering van de klachten kunnen de oorspronkelijke sportactiviteiten weer geleidelijk opgepakt worden. Deze mogen volledig hervat worden wanneer de klachten volledig verdwenen zijn. Om herhaling te voorkomen wordt geadviseerd wordt om de training geleidelijk op te bouwen.
Voorkomen
Het risico op een jumpers knee kan verminderd worden door aandacht te besteden aan het volgende:
Een veel voorkomende oorzaak is overbelasting (te veel, te vaak en te zwaar trainen). Zeker aan het begin van het seizoen is dit een valkuil. Belangrijk is een goede trainingsopbouw waarbij eerst de omvang van de training uitgebreid wordt (het aantal uren) en daarna pas de intensiteit (intensieve oefenvormen met veel loopwerk).
Bosgrond is door zijn dempende werking een ideale ondergrond om op te lopen, zeker wanneer net gestart wordt met lopen.
Kies sportschoenen die geschikt zijn voor de persoonlijke loopstijl en voetvorm. Een goed advies van de speciaalzaak is hierbij heel waardevol. De gemiddelde levensduur van een sportschoen is 500 tot 750 kilometer. Hierna verliest deze snel zijn schokdempende werking.
Soms heeft het lichaam bepaalde tekortkomingen (denk aan X- benen of voetafwijkingen) die deze blessure kunnen veroorzaken. Wanneer deze factoren tijdig worden onderkend en gecorrigeerd, wordt onnodig blessureleed voorkomen.
Wilt u deze informatie downloaden en/of printen? Klik dan hier.
Wil je teruggebeld worden?
Door het invullen van het contactformulier ga je akkoord met onze privacy policy.